

- Refer a Patient
- Referral Types
- Patient Information
- Overview of CFEH Clinics
- CFEH Instrument List
- Our clinical team
- Causes of Vision Loss
- Patient Forms











An Extract from the CFEH Atlas
Bietti Crystalline Corneoretinal Dystrophy
Bietti crystalline corneoretinal dystrophy (BCD) is an autosomal recessive inherited retinal dystrophy characterised by the presence of multiple, refractive crystals in the retina with associated RPE and choriocapillaris atrophy. The crystalline deposits can also be found in the peripheral cornea. It is caused by mutations in the CYP4V2 gene, which is involved in fatty acid metabolism.
BCD is a rare condition but is more common in the East Asian population. The age of onset is usually in the second or third decade of life. Patients with BCD are typically asymptomatic during the earliest stage. As the disease progresses, they start to present with nyctalopia and restricted visual field. Toward the late stage of BCD, severe vision loss and legal blindness are common findings.
Three clinical stages of BCD have been described.
Stage 1 features the presence of refractive crystals in the retina and chorioretinal atrophy lesions limited to the posterior pole. OCT shows the drusen-like structure, loss of the interdigitation zone, and localised disruption of the ellipsoid zone in the macula.
Stage 2: Chorioretinal atrophy expand centrifugally beyond the posterior pole. OCT shows extensive loss of the outer retina and RPE with focal residual RPE and/or EZ in the macula. The crystals tend to disappear but are still been seen at the edge of the atrophic areas.
Stage 3: Diffuse RPE-choriocapillaris complex atrophy is observed throughout the posterior pole. OCT shows extensive loss of outer retina and RPE, and severe atrophy and thinning of the choroid, with the choroidal vessels virtually absent.
Unlike the retinal crystals, the corneal crystals persist in the course of the disease. They are found in the subepithelial and anterior stromal layers and more numerous towards the limbus and do not affect vision.
The diagnosis and staging of BCD are facilitated with multimodal imaging. Colour fundus photograph is useful to image the crystalline deposits, although infrared images are more superior if the crystals are in the intraretinal locations. OCT depicts the crystalline deposits as hyperreflective dots within the retinal layers and displays the disruptions of the retinal and choroidal architectures. Outer retinal tabulation is frequently identified, although it is not specific to BCD and can be found in other inherited retinal dystrophies. FAF is valuable in evaluating the RPE loss.
BCD can be complicated by choroidal neovascularisation and/or macular oedema.
Case Examples
- Case 1
- Case 2
A 58-year-old Asian female with best-corrected visual acuities of 6/12 (20/40) in the right eye and 6/15 (20/50) in the left.
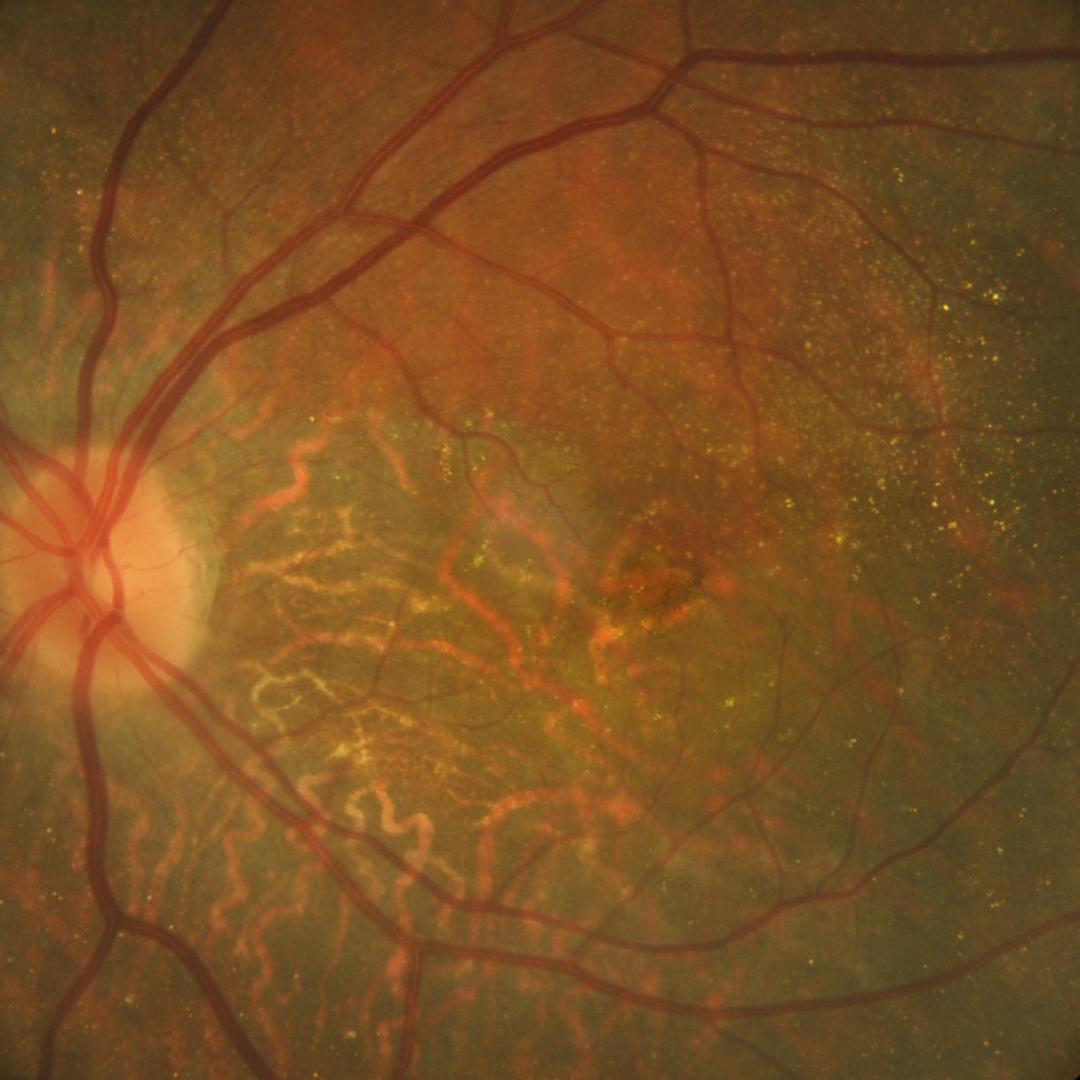
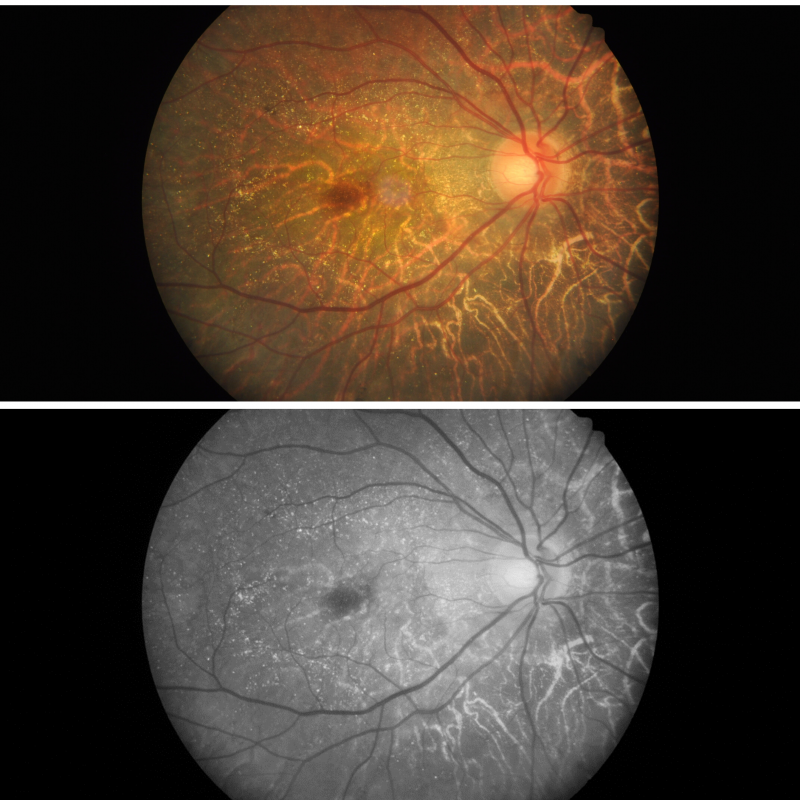
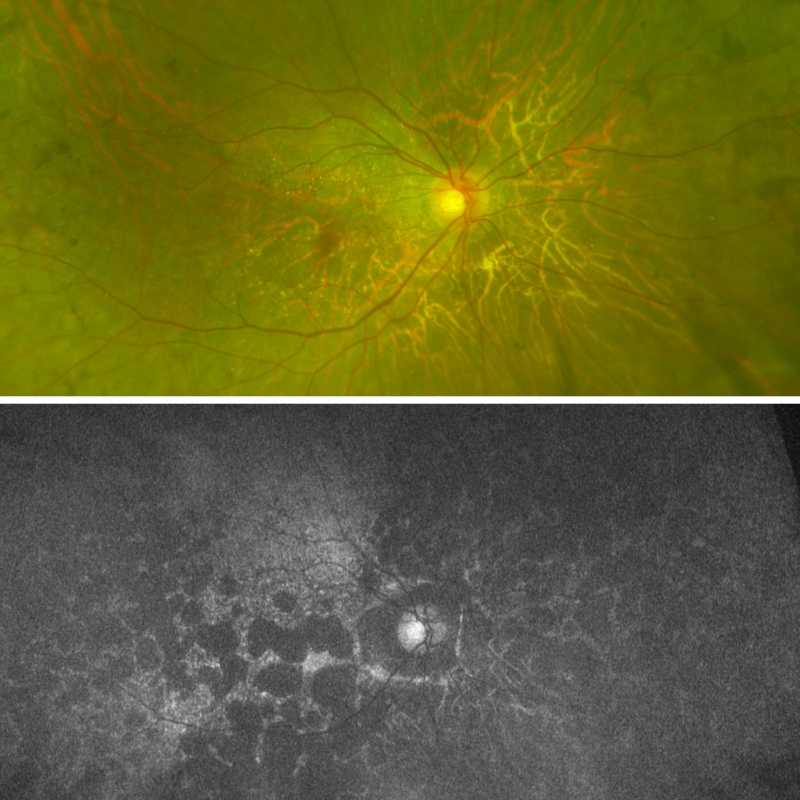
Fundus photograph (OD) shows numerous crystalline deposits in the posterior pole and increased visibility of large choroidal vessels.
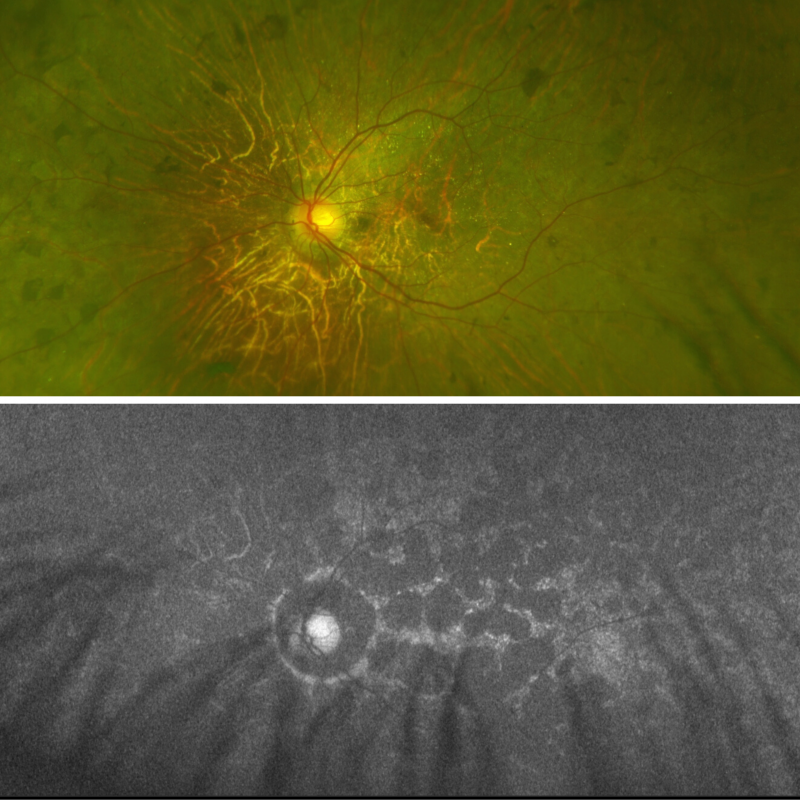
Fundus photograph (OS) shows numerous crystalline deposits in the posterior pole and increased visibility of large choroidal vessels.
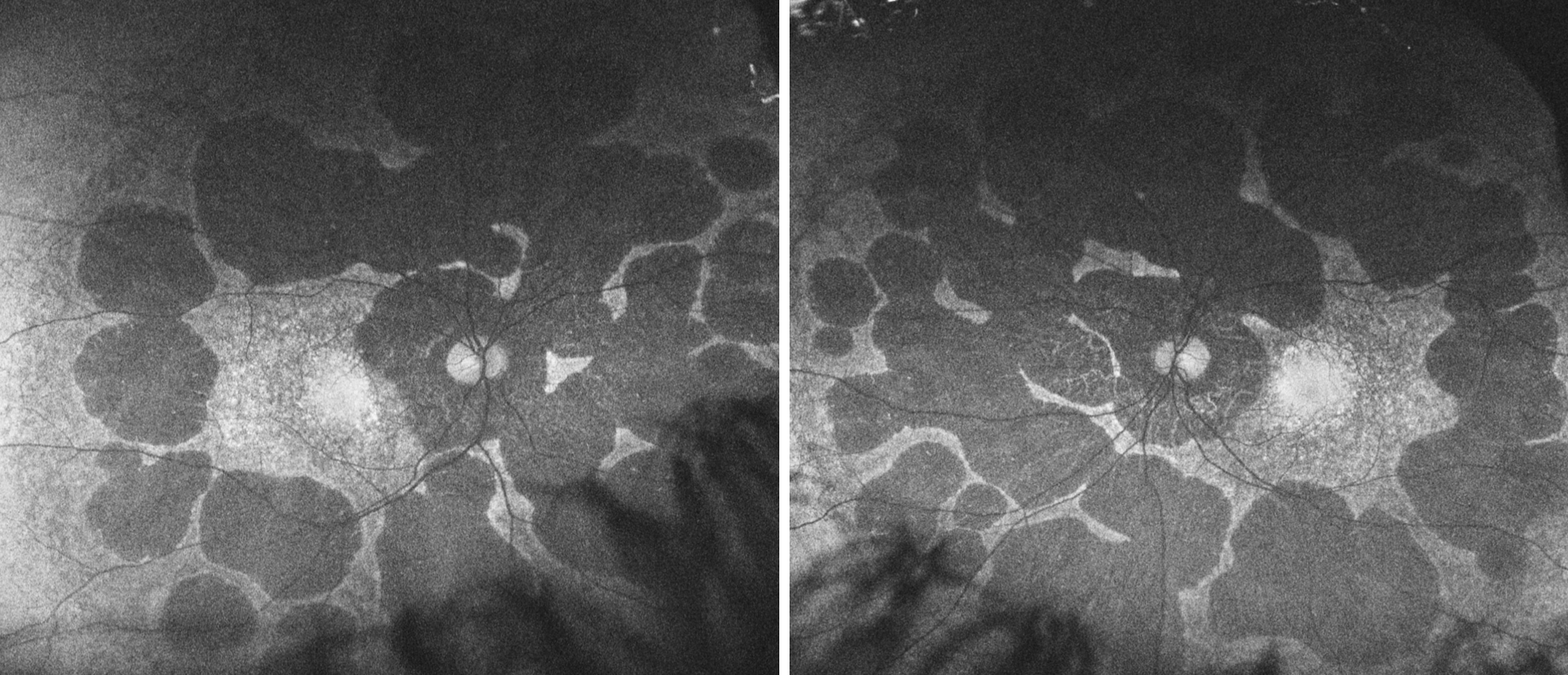
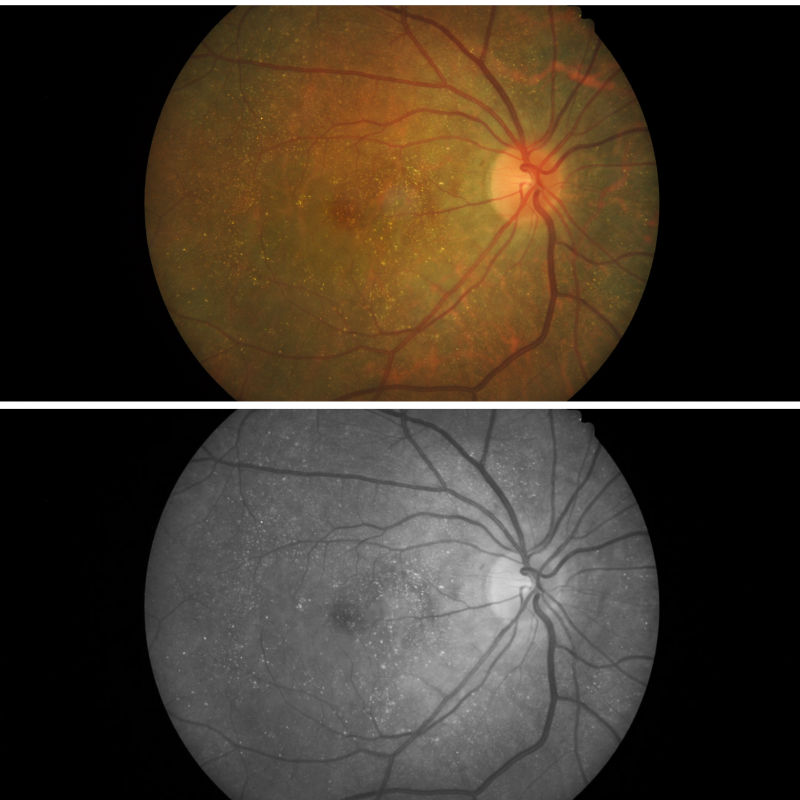
Widefield and fundus autofluorescence (FAF) imaging of the right eye: FAF shows multiple RPE atrophy lesions extend beyond the posterior pole.
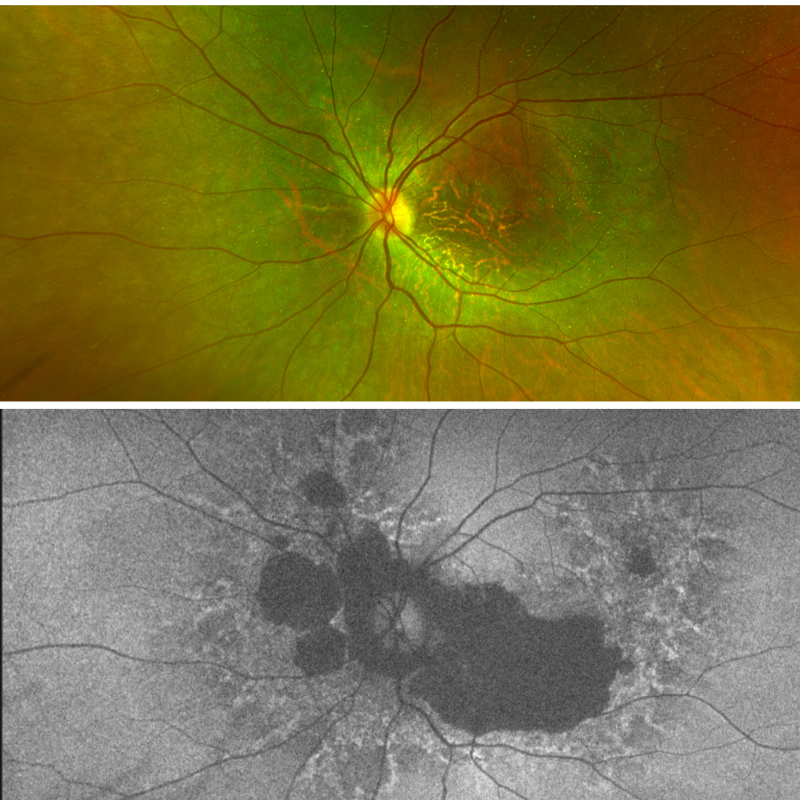
Widefield and fundus autofluorescence (FAF) imaging of the left eye: FAF shows multiple RPE atrophy lesions extend beyond the posterior pole.
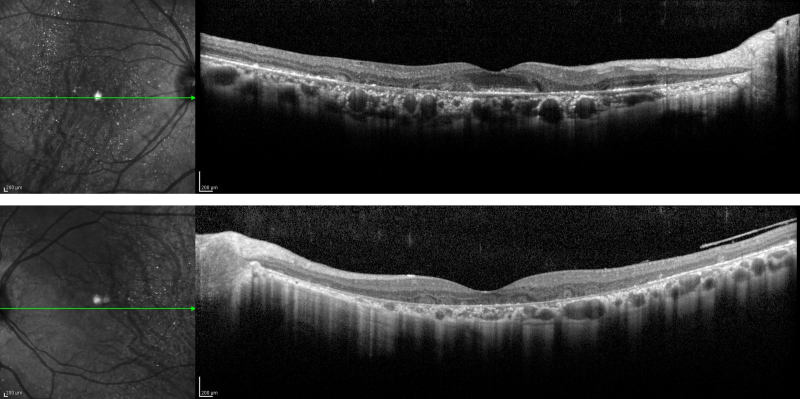
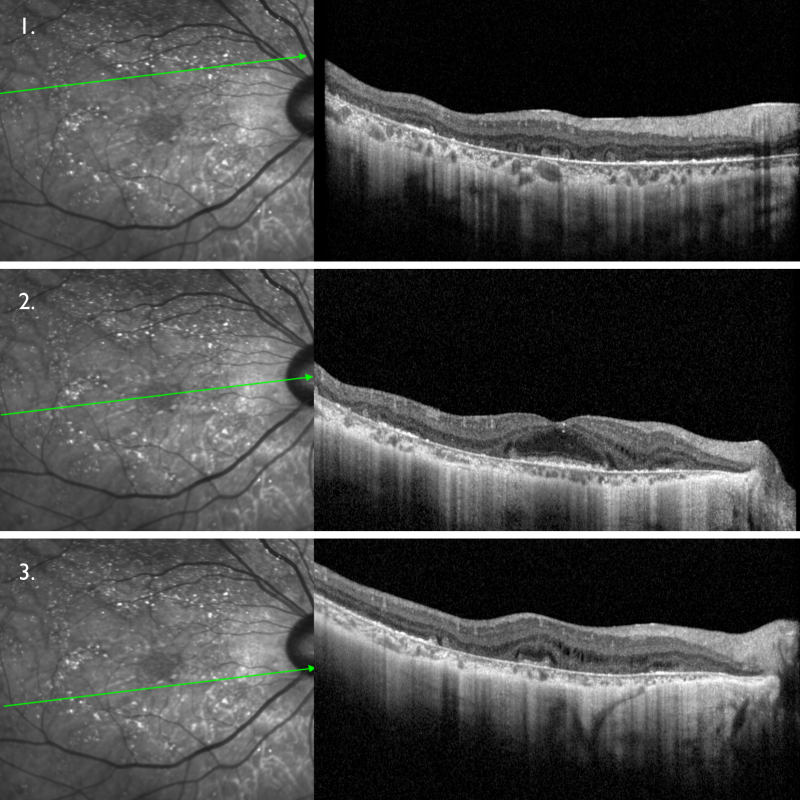
OCT line scans of the right eye show attenuation of outer retina, loss of the ellipsoid zone (EZ) and interdigitation zone, atrophy of the RPE and choriocapillaris corresponding to the profound hypo-autofluorescent regions. Hyperreflective dots corresponding to some of the crystalline deposits are seen primarily in the outer retinal layers. Partial preservation of the EZ and RPE can be seen at the fovea.
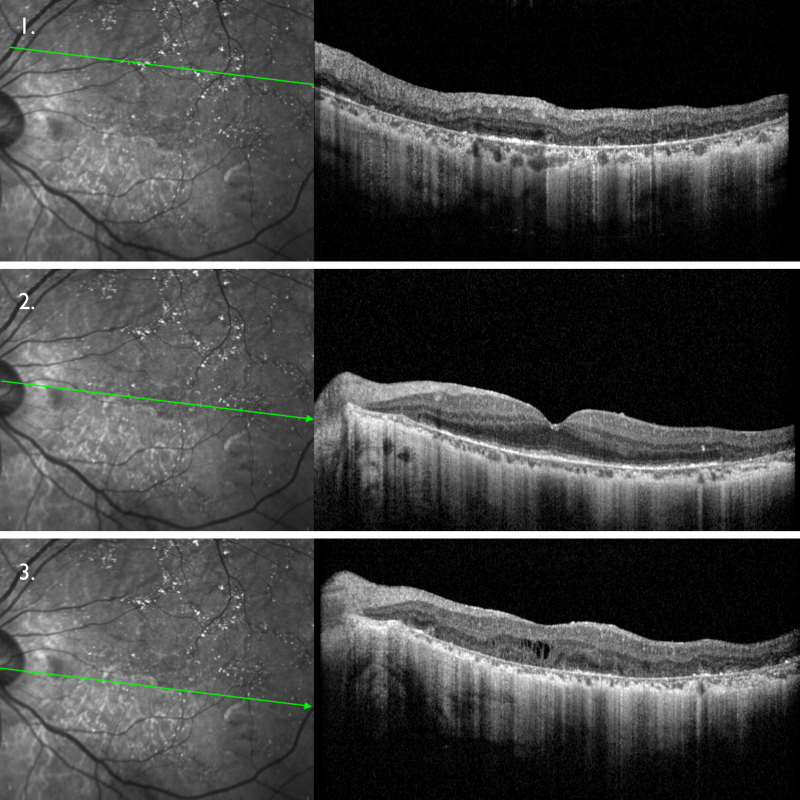
More extensive outer retina attenuation and RPE and choriocapillaris atrophy can be appreciated in the left eye with minimally preserved EZ at the fovea. Outer retinal tubulation is displayed.
A 47-year-old Asian female with visual acuities of 6/6- (20/20-) in the right eye and 6/7.5- (20/25-) in the left.
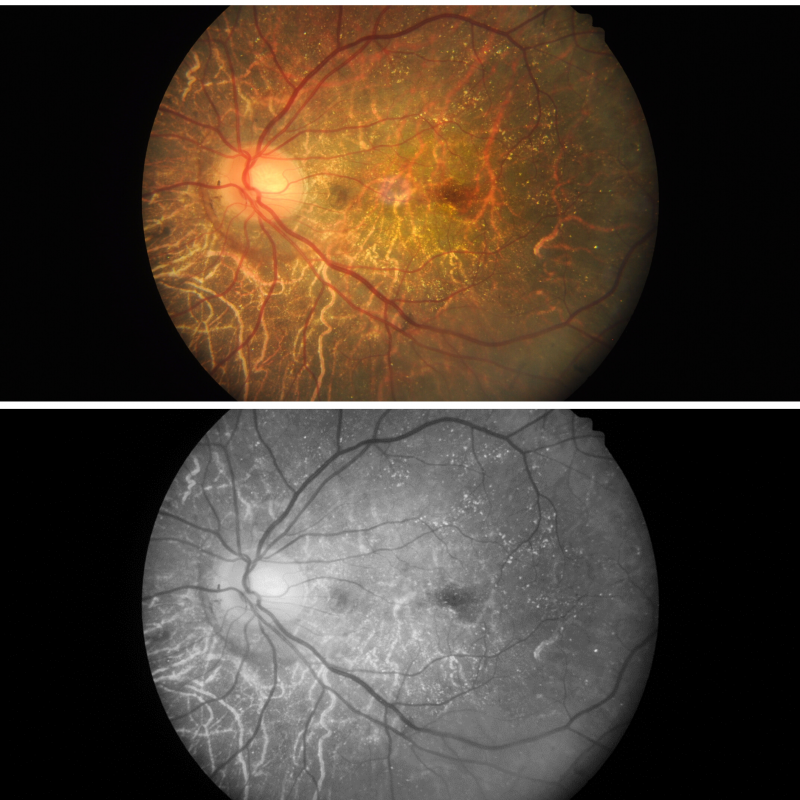
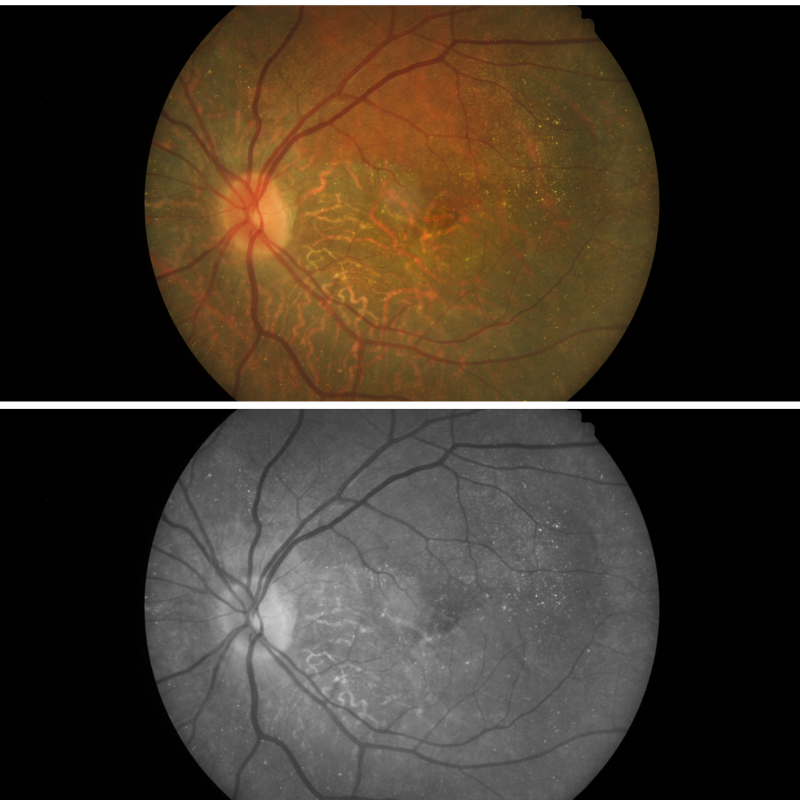
Fundus photographs (and red-free images) show numerous crystalline deposits in the posterior pole and increased visibility of the large choroidal vessels.
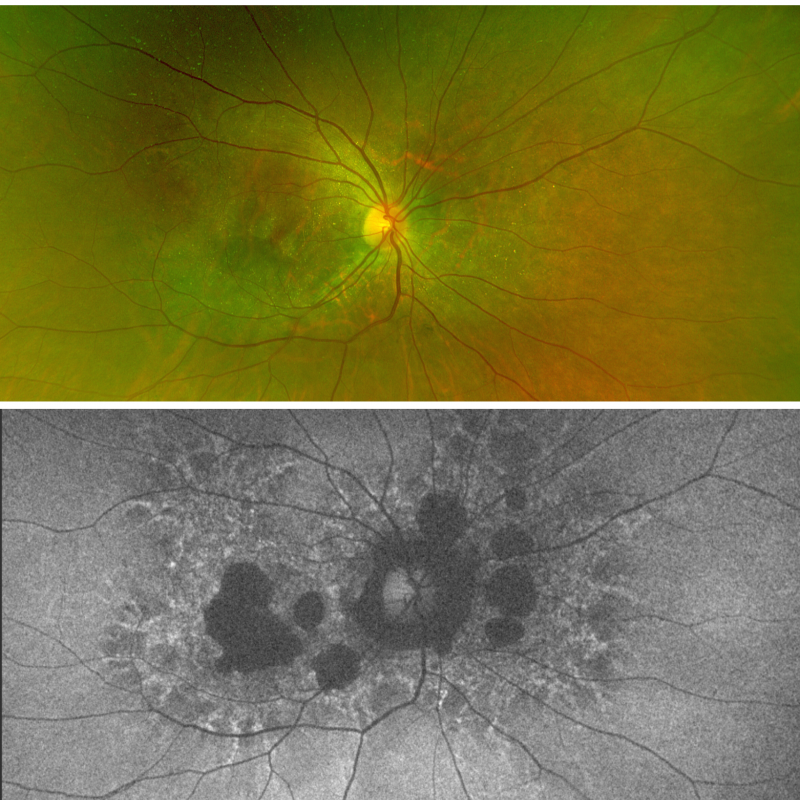
Optomap and fundus autofluorescence images (right eye): FAF shows extensive RPE atrophy involve the posterior pole and midperiphery. Pigment clumping are appreciated in the midperiphery.
Optomap and fundus autofluorescence images (left eye): FAF shows extensive RPE atrophy involve the posterior pole and midperiphery. Pigment clumping are appreciated in the midperiphery.
Spectralis OCT line scans (right eye): OCT line scans show attenuation of outer retina, loss of the ellipsoid zone (EZ) and interdigitation zone, atrophy of the RPE and choriocapillaris. Hyperreflective dots corresponding to some of the crystalline deposits are noted within the retinal layers. Outer retinal tubulation and intra-retinal oedema are also observed. Preservation of the EZ and RPE at the fovea may explain the relatively good visual acuity.
Spectralis OCT line scans (left eye): OCT line scans show attenuation of outer retina, loss of the ellipsoid zone (EZ) and interdigitation zone, atrophy of the RPE and choriocapillaris. Hyperreflective dots corresponding to some of the crystalline deposits are noted within the retinal layers. Outer retinal tubulation and intra-retinal oedema are also observed. Preservation of the EZ and RPE at the fovea may explain the relatively good visual acuity.
Differential Diagnosis
Another differential to consider is Central Areolar Choroidal Dystrophy. More information on this condition may be found in the CFEH Atlas.
Other conditions to consider with a crystalline retinopathy include cystinosis, hyperornithinemia, talc retinopathy, Alport syndrome, Sjögren-Larsson syndrome, macular telangiectasia, canthaxanthin toxicity and tamoxifen retinopathy
References
García-García GP, Martínez-Rubio M, Moya-Moya MA et al. Current perspectives in Bietti crystalline dystrophy. Clinical ophthalmology (Auckland, NZ) 2019; 13: 1379-1399.
Yuzawa M, Mae Y, Matsui M. Bietti’s crystalline retinopathy. Ophthalmic paediatrics and genetics 1986; 7: 9-20.
Oishi A, Oishi M, Miyata M et al. Multimodal Imaging for Differential Diagnosis of Bietti Crystalline Dystrophy. Ophthalmol Retina 2018; 2: 1071-1077.
Wang W, Chen W, Bai X et al. Multimodal imaging features and genetic findings in Bietti crystalline dystrophy. BMC Ophthalmol 2020; 20: 331.
Yin H, Jin C, Fang X et al. Molecular analysis and phenotypic study in 14 Chinese families with Bietti crystalline dystrophy. PloS one 2014; 9: e94960-e94960.